
💡 Key Points to Remember
- Clinical Calculations: Embedded in clinical scenarios, not standalone.
- Focus Area: Allocate 50% effort on Therapeutics & Patient Care.
- Core Skills: Master unit conversions, CrCl, BSA, IV rates, and dilutions.
- Plausibility Check: Always verify your answers before final submission.
- Daily Practice: 15–30 mins builds speed, accuracy, and confidence.
- Expert Insight: Learn from experienced Australian pharmacists for real-world reasoning.
Imagine This
The sun is just beginning to rise over the Yarra River, casting a soft glow across the Northern Health ward. You step into the bustling dispensary for your morning shift, the faint hum of monitors and the occasional clatter of trolleys filling the air. Your senior clinical pharmacist, Arief Mohammad, approaches and hands you a patient chart.
“This patient is 78 years old, weighs 54 kg, and has a serum creatinine of 195 µmol/L,” he says, eyes steady behind his glasses. “We need to start enoxaparin. Tell me the creatinine clearance, and recommend the safest dose.”
In that moment, pharmacy calculations stop being abstract numbers on paper.
They become decisions that could affect real lives. This is exactly what the OPRA exam tests.
In 2026, under the Australian Pharmacy Council (APC) framework, calculations are no longer standalone math problems. They are embedded within clinical scenarios, particularly in the Therapeutics & Patient Care domain.
You are not simply solving for X, you are evaluating patient safety, weighing risk, and making informed decisions.
This guide breaks down OPRA pharmacy calculations the way top-scoring candidates at Elite Expertise learn them: how to think, how to practice, and how to apply formulas safely in realistic clinical contexts, with a structured daily framework that builds both speed and confidence.
Why OPRA Calculations Are Different from KAPS
Under the Australian Pharmacy Council (APC) framework, calculations are no longer standalone math problems. They are embedded within clinical scenarios, particularly in the Therapeutics & Patient Care domain.
You are not simply solving for X—you are evaluating patient safety, weighing risk, and making informed decisions.
This guide breaks down OPRA pharmacy calculations the way top-scoring candidates at Elite Expertise learn them:
- How to think
- How to practice
- How to apply formulas safely in realistic clinical contexts
- Structured daily framework that builds both speed and confidence
Why OPRA Calculations Are Different from KAPS
Under the old KAPS format, pharmacy calculations were usually standalone, predictable and heavily memorisation-based. You were often given a direct formula, clear numbers and a single correct answer with little clinical context. Many candidates prepared by drilling question banks and memorising patterns.
OPRA has changed that approach completely.
What OPRA Tests Instead
OPRA is designed to assess how you think as a pharmacist and not how fast you calculate. Calculations are now used to test:
- Clinical reasoning
- Risk prioritisation
- Dose safety
- Real-world plausibility
Instead of isolated maths questions, calculations are embedded inside case-based MCQs. You may first need to understand the patient scenario before deciding whether a calculation is even appropriate. These scenarios commonly involve:
- Renal impairment and dose adjustments
- Elderly patients with multiple comorbidities
- Paediatric weight-based dosing
- IV infusions and dilution safety
- High-risk medicines with narrow therapeutic windows
Because OPRA uses Rasch-based scoring, accuracy and consistency matter more than attempting every question. A single decimal error or unsafe dose can outweigh several correct recall-based answers. This is why pharmacy calculations are considered a high-return scoring area but only when trained with clinical context and safety awareness.
Common OPRA Clinical Scenarios
- Renal impairment and dose adjustments
- Elderly patients with multiple comorbidities
- Paediatric weight-based dosing
- IV infusions and dilution safety
- High-risk medicines with narrow therapeutic windows
Because OPRA uses Rasch-based scoring, accuracy and consistency matter more than attempting every question. A single decimal error or unsafe dose can outweigh several correct recall-based answers.
Dose Calculations and Conversions (Foundation Skill)
Metric Conversions (Rule of 1000)
- 1 g = 1,000 mg
- 1 mg = 1,000 microg
- 1 microg = 1,000 ng
Clinical safety note: In Australia, “micrograms” is written in full or as microg. The symbol µg is avoided to prevent confusion with mg.
Weight-Based Dosing
Common OPRA formats:
- mg/kg/day
- mg/kg/dose
- Maximum dose limits
Always double-check:
- Patient weight
- Age
- Renal function
- Whether the dose is per dose or per day
Many candidates lose marks not because of poor maths but because they misread the clinical context.
Creatinine Clearance (CrCl): The Most Tested Calculation
Renal dosing is one of the highest-yield calculation areas in the OPRA exam because impaired kidney function directly affects drug safety. OPRA repeatedly tests whether you can identify risk and adjust therapy, not just apply a formula mechanically.
You must be fluent with the Cockcroft–Gault equation, as this is the method most commonly used in Australian clinical practice and aligns with how pharmacists assess renal function for dose decisions.
Cockcroft–Gault Formula
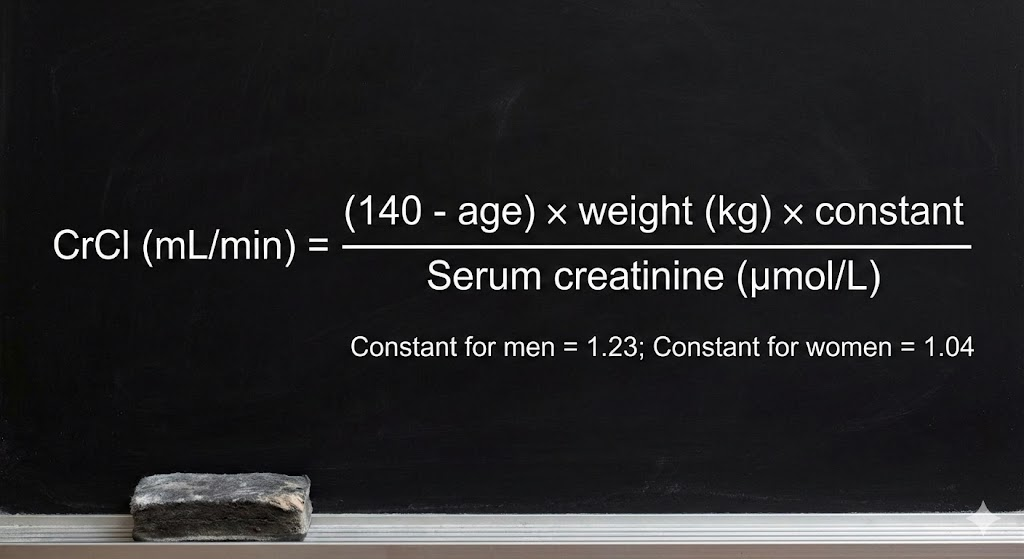
Fluency required: Cockcroft–Gault equation (commonly used in Australian practice).
However, OPRA does not reward candidates who stop at the final number.
How OPRA Tests CrCl
OPRA commonly links CrCl to:
- Dose reduction requirements
- Frequency adjustments
- Drug contraindications
- Choosing the safest option rather than the most aggressive therapy
You may be asked to decide whether a medicine should be continued, reduced, switched, or avoided entirely based on renal function and patient factors such as age and comorbidities.
At Elite Expertise, Arief Mohammad (Arief Sir) emphasises clinical interpretation over calculation speed:
“The number means nothing unless you know what it changes.” – Arief Mohammad
IV Flow Rates and Dilution (Hospital-Focused Calculations)
OPRA frequently places candidates in hospital, ward, or emergency department scenarios, where IV calculations are not just mathematical exercises but patient-safety decisions. These questions test whether you can remain accurate under pressure exactly how Australian pharmacists are expected to function in clinical settings.
Drip Rate Calculations (gtt/min)
Drip rates are used when gravity infusions are described instead of infusion pumps.
Formula:
Drip rate (gtt/min) = (Volume in mL × Drop factor in gtt/mL) ÷ Time in minutes
- The drop factor is always provided in the question, commonly 20 gtt/mL (macrodrip) or 60 gtt/mL (microdrip). Your role is to apply it correctly and avoid mixing minutes with hours, a common exam trap.
Infusion Pump Rate (mL/hr)
Example: 250 mL over 2 hours → 125 mL/hr
OPRA tests this in high-stress clinical contexts. Rushing leads to errors; unsafe dosing is penalised.
Dilution Calculations: C₁V₁ = C₂V₂
- High-risk, high-yield in OPRA
- Common medicines: Potassium chloride, adrenaline, highly concentrated stocks
- Safety: Precision is critical; errors are considered critical safety breaches
Millimoles and Electrolytes
Scenario:
- Potassium level: 2.8 mmol/L
- Doctor orders: 40 mmol KCl as slow infusion
- Ampoules: 10 mL KCl labeled 1.49 g/10 mL
Step-by-Step:
- Molecular Weight: K = 39, Cl = 35.5 → MW = 74.5 g/mol
- 1 mmol KCl = 74.5 mg
- Total mg needed: 40 mmol × 74.5 mg/mmol = 2980 mg ≈ 3 g
- Ampoules required: 3 g ÷ 1.49 g ≈ 2 ampoules
Displacement Volumes: Reconstitution Precision
Scenario: Amoxicillin
- Bottle requires 82 mL water to make 100 mL suspension (250 mg/5 mL)
Step-by-Step:
- Total suspension volume = 100 mL
- Water added = 82 mL
- Displacement volume = 100 – 82 = 18 mL
Adding only 80 mL changes the concentration. OPRA tests practical reasoning and patient safety.
Concentrations, Ratios, and Percentages
- Percent strength (w/v) = grams per 100 mL
- Example: 0.9% sodium chloride → 0.9 g/100 mL → 9 mg/mL
- Ratio strengths:
- Adrenaline 1:1,000 = 1 mg/mL
- Adrenaline 1:10,000 = 0.1 mg/mL
Confusing ratios can be fatal; OPRA tests clinical pause, not just mechanical calculation.
Sensitivity Checks (Plausibility)
Elite Expertise habit: Always ask before finalizing:
- Is this dose physically possible?
- Is it clinically reasonable?
- Is it safe for the patient or nurse?
Common Red Flags:
- 20+ tablets in a single dose
- Paediatric doses higher than adult
- Large IM injection volumes
- Extremely fast or slow infusion rates
“Your brain knows when something feels unsafe—listen to it.” – Harika Bheemavarapu
Daily Practice Routine (15–30 Minutes)
- 0–5 min: Unit Conversions (mg ↔ microg ↔ g)
- 5–15 min: Core Three Calculations
- Creatinine clearance (CrCl)
- IV infusion rate
- Dilution calculation
- 15–25 min: Case-Based Calculation (therapeutics-linked)
- 25–30 min: Plausibility Check & Review
How Elite Expertise Trains OPRA Calculations Differently
Challenges with self-study:
- Formulas practiced without context
- Errors repeated without feedback
- Safety reasoning missing
Why Elite Expertise Works:
- OPRA-focused curriculum
- Rasch-aligned mock tests
- Scenario-based teaching
Meet the Trainers
Mr. Arief Mohammad
- Clinical Pharmacist – Northern Health, Melbourne
- AACPA Accredited Consultant Pharmacist
- Specialises in ward-level reasoning, renal dosing, risk prioritisation
Mrs. Harika Bheemavarapu
- Clinical Pharmacist – Monash Health, Melbourne
- AACPA Accredited Consultant Pharmacist
- Focuses on step-by-step calculation logic, pharmaceutical sciences, confidence-building
Together, they teach how Australian pharmacists think, not just how they calculate.
OPRA Calculations: What NOT to Use
- AMH, eTG, and APF are NOT OPRA calculation resources
- They are used for: Intern Written Exam, Internship practice
- OPRA focuses on: Conceptual understanding, safe decision-making, logical reasoning
Final Takeaway
OPRA pharmacy calculations are not about speed maths.
They are about:
- Accuracy
- Context
- Safety
- Reasoning under pressure
With a structured practice framework and guidance from practising Australian pharmacists, calculations become one of your strongest scoring areas.
If you train the Elite way, thinking clinically, checking plausibility and practising consistently, you don’t just pass OPRA.
You prove you are ready to practise pharmacy in Australia.